
Severe period pain is often dismissed as “normal,” but pain that disrupts your daily life should not be ignored. While mild menstrual cramps are common, intense pain that causes you to miss work, school, exercise, or social activities may be a sign of an underlying women’s health condition such as endometriosis.
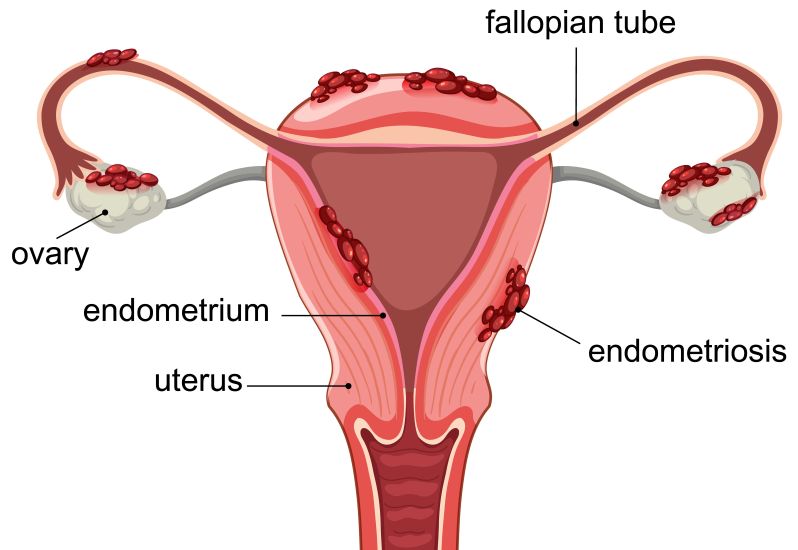
Endometriosis is a chronic disease where tissue similar to the lining of the uterus grows outside the uterus. This endometriosis tissue may affect the pelvic organs, reproductive organs, ovaries, fallopian tubes, bowel, bladder, and pelvic tissues. It can cause inflammation, scar tissue, chronic pain, and fertility difficulties. The World Health Organization estimates that endometriosis affects about 10% of women and girls of reproductive age worldwide.
If you are trying to understand endometriosis symptoms, the possible causes of endometriosis, or the right endometriosis treatment, the most important thing to know is this: endometriosis can look very different from person to person. Some people experience severe pain, while others have little or no pain and may only be diagnosed when they seek help for fertility concerns.
Endometriosis Symptoms That People Often Miss
Endometriosis symptoms can be easy to miss because they often overlap with “normal” period discomfort, digestive problems, urinary symptoms, or other pelvic conditions. Some people are told for years that their painful periods are just part of the menstrual cycle, even when the pain is severe enough to affect daily life.
Common endometriosis symptoms
Common symptoms of endometriosis include:
- Painful periods or painful menstrual cramps
- Pelvic pain, especially before or during menstrual periods
- Abdominal pain or lower back pain
- Pain during sex
- Pain with bowel movements
- Pain during urination, especially during periods
- Heavy bleeding or excessive bleeding
- Spotting between periods
- Bloating, sometimes described as “endo belly”
- Bowel and bladder symptoms, such as diarrhoea, constipation, nausea, or bladder discomfort
- Fatigue, including persistent exhaustion that does not improve with rest
- Fertility difficulties
Pelvic pain is one of the most common symptoms of endometriosis. It may start several days before a period and continue during menstruation. Some people also experience referred pain that spreads to the lower back, hips, or legs.
The pain does not always match the amount of endometriosis lesions present. A person with severe endometriosis may have mild symptoms, while someone with smaller or superficial peritoneal endometriosis may experience intense pain. This is why symptoms should be taken seriously even when scans do not show obvious disease.
Symptom patterns that raise suspicion
Endometriosis may be suspected when symptoms follow a cyclical pattern, especially when they worsen before or during menstrual periods. Gastrointestinal or urinary symptoms that appear around the period can also be a clue.
Symptoms that raise suspicion include:
- Pain that disrupts work, school, sleep, or normal activities
- Pain that gets worse over time
- Pain with bowel movements or urination during periods
- Pelvic pain that happens outside the period
- Heavy or irregular bleeding together with pelvic pain
- Painful sex, especially deep pelvic pain
- Severe menstrual cramps that are not relieved by standard over-the-counter painkillers
Endometriosis can sometimes be mistaken for other conditions, including irritable bowel syndrome, pelvic inflammatory disease, ovarian cysts, or bladder-related conditions. A proper medical evaluation can help narrow down the cause of symptoms and avoid unnecessary delays in care.
Causes of Endometriosis and Why the Exact Cause Is Still Unclear
What we know about the causes of endometriosis
The exact cause of endometriosis is still not fully known. Current evidence suggests that several factors may be involved rather than one single cause. These may include menstrual blood flow patterns, genetic factors, immune system changes, hormonal influence, and how certain cells behave inside the pelvic cavity.
Endometriosis happens when endometrial-like tissue grows outside the uterus. This tissue acts in some ways like the uterine lining: it can respond to hormones during the menstrual cycle, leading to inflammation, irritation, bleeding, scar tissue, and adhesions. Adhesions can cause pelvic tissues or pelvic organs to stick together, contributing to pain and fertility problems.
Commonly discussed contributing factors
Several theories and risk factors are commonly discussed when explaining the causes of endometriosis.
- Retrograde menstruation
Retrograde menstruation occurs when menstrual blood flows backwards through the fallopian tubes into the pelvic cavity instead of leaving the body fully through the vagina. This may allow endometrial cells to reach pelvic organs and pelvic tissues. However, retrograde menstruation alone does not explain every case, because many people may have backward menstrual blood flow without developing endometriosis. - Genetics and family history
Endometriosis may be more likely in people with a family history of the condition. This suggests that inherited factors may contribute to the risk of developing endometriosis. - Immune system factors
The immune system may play a role in whether endometrial-like cells are cleared from the body or allowed to implant and grow. Immune system dysfunction is one of the commonly discussed factors for endometriosis. - Hormonal influence
Estrogen can encourage endometriosis tissue growth. This is why many hormone treatments aim to reduce or control the hormonal stimulation of endometriosis lesions. - Cell transformation theories
Some theories suggest that cells outside the uterus, such as peritoneal cells in the pelvic cavity, may transform into endometrial-like cells. This is sometimes discussed as coelomic metaplasia.
Risk factors may include never giving birth, starting periods at an early age, short menstrual cycles, heavy menstrual periods, higher estrogen exposure, low body mass index, and family history. However, having one or more risk factors does not mean someone will definitely develop endometriosis.
Why do symptoms vary so much from person to person
Endometriosis symptoms vary because the condition can affect different areas of the body. Lesions may be found on the ovaries, fallopian tubes, pelvic lining, bowel, bladder, or other pelvic organs. Some people develop ovarian endometriomas, also called chocolate cysts. Others may have superficial peritoneal endometriosis or deep infiltrating endometriosis, where tissue grows more deeply into pelvic structures.
Symptoms may also depend on inflammation, scar tissue, adhesions, nerve involvement, and individual pain sensitivity. This explains why the level of pain does not always correlate with the visible extent of endometriosis tissue.
Endometriosis Treatment Options and What They Aim to Do
What endometriosis treatment is designed to do
There is currently no absolute cure for endometriosis. Endometriosis treatment focuses on helping patients manage symptoms, reduce pain, improve quality of life, support fertility goals where relevant, and reduce the risk of recurrence where possible.
Treatment for endometriosis is usually personalised. The right treatment plan depends on symptom severity, age and life stage, pregnancy plans, previous treatment response, and access to specialist care.
Main endometriosis treatment options
Endometriosis treatment options may include pain relief, hormone therapy, surgery, fertility treatment, or a combination approach.
- Pain relief medicines
Pain relief may include non-steroidal anti-inflammatory drugs or other medicines recommended by a doctor. These may help relieve pain, especially for mild symptoms. However, standard over-the-counter painkillers may not adequately control severe endometriosis pain. - Hormonal birth control and hormone treatments
Hormone therapy may help manage symptoms by controlling hormonal changes during the menstrual cycle. Options may include hormonal contraceptives, oral contraceptive pills, progestins, or injections that create a temporary menopause-like state. These medical treatments may reduce pain and slow disease activity, but they do not permanently remove endometriosis tissue. - Surgical treatment
Surgical treatment may be considered when symptoms are severe, medical treatments are not effective, fertility is affected, or an endometriosis diagnosis requires further confirmation. Minimally invasive surgery, usually laparoscopy, may be used to diagnose endometriosis and remove endometriosis lesions, scar tissue, or endometriomas. - Combination approach
Some patients benefit from a combination of surgery and hormone therapy, especially when the goal is to relieve symptoms and reduce recurrence risk. The best combination depends on symptoms, fertility plans, and the type and location of the disease. - Fertility treatment
Endometriosis can affect fertility by causing inflammation, scar tissue, distortion of the fallopian tubes, ovarian endometriomas, and changes that may affect eggs, sperm, embryo implantation, or the pelvic environment. Some patients may need fertility treatment, depending on age, ovarian reserve, severity of disease, and how long they have been trying to conceive. ASRM notes that classical studies suggest 25% to 50% of infertile women have endometriosis, although the true prevalence varies widely.
In selected cases, hysterectomy may be discussed for women with severe symptoms who have completed their family or are near menopause. However, hysterectomy is not suitable for everyone and does not guarantee that all pain will disappear, especially if endometriosis remains outside the uterus.
How treatment decisions are usually made
Doctors usually consider several factors before recommending how to treat endometriosis, including:
- How severe the pain is
- Whether symptoms affect daily life, work, school, sleep, or relationships
- Whether bowel and bladder symptoms are present
- Whether heavy bleeding or excessive bleeding is occurring
- Whether the patient is trying to conceive
- Whether fertility treatment may be needed
- Whether previous hormone treatments or pain relief medicines helped
- Whether imaging suggests endometriomas, deep infiltrating endometriosis, or other pelvic disease
Early treatment of endometriosis may help some patients manage symptoms better and reduce long delays in care. Early diagnosis is especially important when pain is worsening, fertility is affected, or symptoms do not match a “normal cramp” pattern.
When to See a Doctor for Possible Endometriosis
Book an appointment if:
You should consider booking an appointment with the expert gynaecologist if:
- Period pain is severe or worsening
- Pain affects work, school, sleep, or daily function
- Pelvic pain happens outside your period
- Heavy bleeding and pelvic pain happen together
- Pain occurs during sex
- Pain occurs with bowel movements or urination during periods
- Bloating, diarrhoea, constipation, nausea, or bladder symptoms happen cyclically
- You have difficulty conceiving after one year of unprotected intercourse, or after six months if you are over 35
Infertility can sometimes be the first sign of endometriosis, especially in people with silent endometriosis who have little or no pain. Many people with endometriosis can still become pregnant, but the condition may affect fertility in some cases.
Seek urgent care if:
Seek urgent medical care if you experience:
- Sudden and intense severe pain
- Heavy bleeding with dizziness, weakness, or fainting
- Severe pelvic pain with fever or vomiting
- Severe pain with a positive pregnancy test
- Symptoms that feel unusual, sudden, or much worse than your normal period pain
Urgent symptoms are not always caused by endometriosis. They may also be linked to other conditions that need prompt assessment, such as ovarian cyst complications, infection, ectopic pregnancy, or pelvic inflammatory disease.
What to Expect During Evaluation
Questions clinicians may ask
During evaluation, your doctor may ask about:
- When the pain starts and how long it lasts
- Whether pain is linked to the menstrual cycle
- Whether pain happens during sex, bowel movements, or urination
- Whether bleeding is heavy, prolonged, irregular, or includes spotting
- Whether you have bowel and bladder symptoms
- Whether you experience fatigue, bloating, or chronic pain
- Whether symptoms are affecting your mental health or daily life
- Whether you have fertility concerns
- Whether there is a family history of endometriosis
Bringing a symptom diary can help. Try to record your cycle dates, pain severity, bleeding pattern, bowel symptoms, bladder symptoms, medication use, and days when symptoms affect normal activities.
Common tests and assessments
Endometriosis is diagnosed properly, usually beginning with a careful symptom history and clinical review. A pelvic exam may be performed when appropriate. Ultrasound may be used to assess the uterus, ovaries, endometriomas, and other pelvic findings. In selected cases, other imaging such as MRI or specialist review may be recommended.
It is important to know that a normal ultrasound does not always rule out endometriosis. Some forms, especially superficial peritoneal endometriosis, may not be clearly visible on standard imaging. Current guidelines increasingly support a clinical and imaging-based approach, with laparoscopy considered when imaging is negative, symptoms persist, empirical treatment is unsuitable, or fertility-related decision-making requires more certainty.
Laparoscopy allows a doctor to look inside the pelvic cavity and, where appropriate, remove or biopsy suspected endometriosis lesions. In many settings, laparoscopy with tissue confirmation is still used to definitively diagnose endometriosis, especially when the diagnosis remains uncertain or surgical treatment is being planned.
When Period Pain Is More Than Period Pain
Endometriosis symptoms go beyond ordinary cramps. They may include pelvic pain, painful periods, pain during sex, bowel and bladder symptoms, abdominal pain, bloating, fatigue, heavy bleeding, chronic pain, and fertility difficulties.
The causes of endometriosis are multifactorial and still not fully understood. Retrograde menstruation, genetics, immune system changes, estrogen, peritoneal cell transformation, inflammation, and other factors may all play a role.
Endometriosis treatment focuses on long-term symptom control, quality of life, fertility goals, and recurrence risk. Some patients may benefit from pain relief and hormone therapy, while others may need minimally invasive surgery, fertility treatment, or a combination treatment plan.
If your period pain feels severe, worsening, or different from normal cramps, you do not need to manage it alone. Book a consultation with Dr Law Wei Seng to discuss your symptoms, receive a proper endometriosis diagnosis, and explore a treatment plan that fits your health and future goals.
Frequentley Asked Questions
What are the first signs of endometriosis?
The first signs of endometriosis may include painful periods, pelvic pain before or during menstruation, pain during sex, pain with bowel movements or urination during periods, heavy bleeding, bloating, fatigue, or difficulty conceiving. Some people have little or no pain and are only diagnosed after seeking help for infertility.
Can endometriosis symptoms be mistaken for normal period pain?
Yes. Endometriosis symptoms are often mistaken for normal period pain, especially when painful menstrual cramps are treated as something that must simply be tolerated. Pain that disrupts daily activities, worsens over time, occurs outside the period, or is not relieved by usual painkillers should be assessed by a doctor.
What causes endometriosis?
The exact cause of endometriosis is unknown. Possible contributing factors include retrograde menstruation, family history, immune dysfunction, hormonal influences, and transformation of pelvic cavity cells into endometrial-like cells. Most experts consider endometriosis a multifactorial condition rather than a disease with one single cause.
What is the best endometriosis treatment?
There is no single best endometriosis treatment for everyone. Treatment options may include pain relief medicines, hormonal birth control, progestins, hormone therapy, surgical treatment, minimally invasive surgery, fertility treatment, or a combination approach. The best option depends on symptoms, age, pregnancy plans, disease location, previous treatment response, and personal goals.
Can endometriosis come back after treatment?
Yes. Endometriosis symptoms can recur after treatment, especially because it is a chronic disease. Surgery can remove visible endometriosis tissue and may relieve symptoms, but it does not always permanently prevent recurrence. Long-term management may include follow-up care, hormone treatments where suitable, pain management, and review of fertility goals.